What is Chronic Lymphocytic Leukemia (CLL)?
Chronic Lymphocytic Leukemia (CLL) is the most common type of leukemia diagnosed in adults. It is a cancer of the B-lymphocyte. In rare cases, CLL may be hereditary, but most causes are unknown. The stage of CLL can vary at diagnosis and throughout treatment. Stages of CLL include Rai stage 0, I, II, III, or IV. Many therapies are not curative, however, newer therapies are able to suppress the cancer for many months or even years.
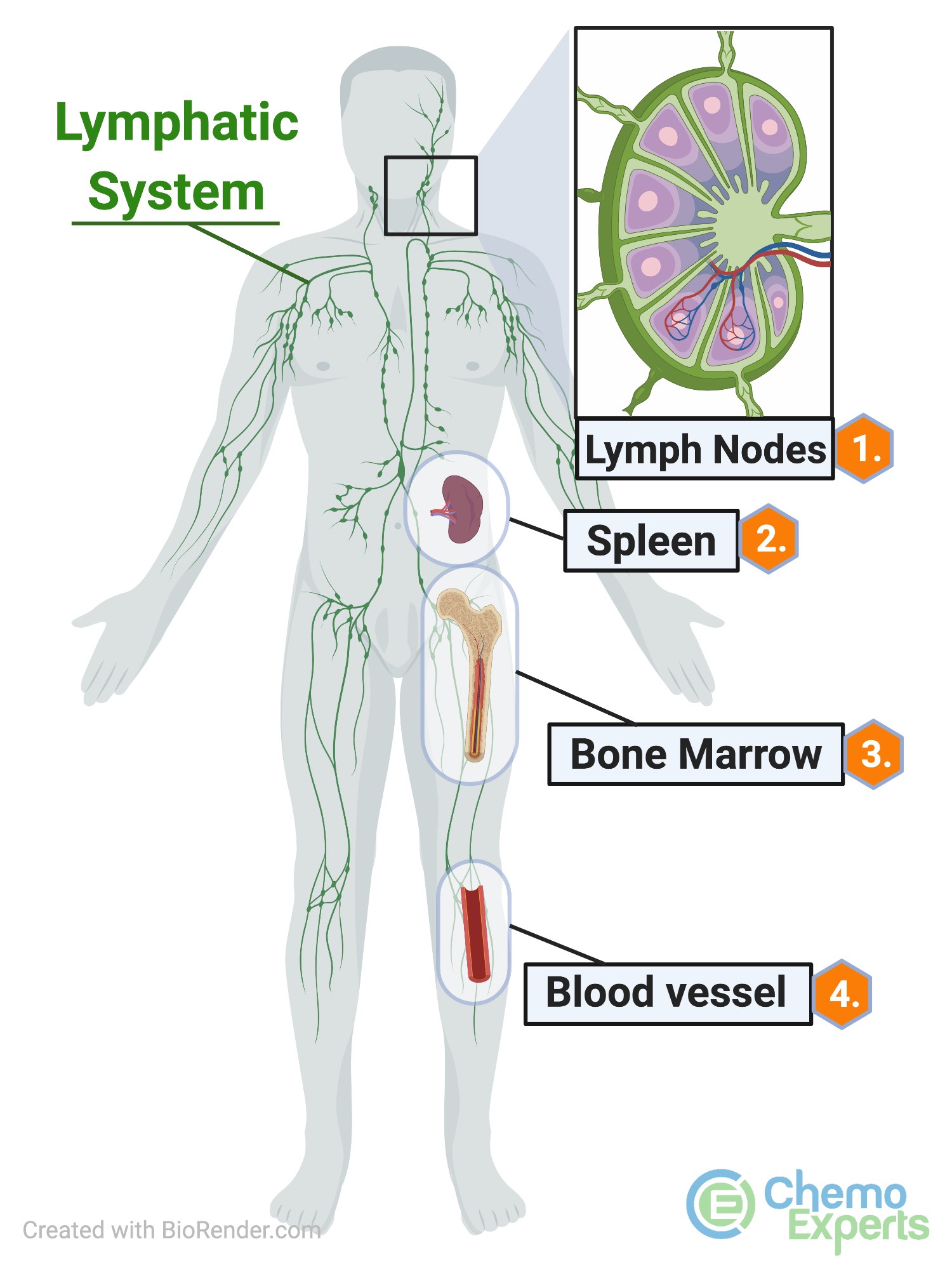
As depicted in the picture, CLL may affect lymph nodes, the spleen, bone marrow, and the blood.
Medications for CLL may include intravenous infusions, oral tablets or capsules, or a combination of IV and oral medications. Patients may be diagnosed with CLL without having any symptoms. Others may go to their doctor with symptoms of fatigue, a large spleen, or decreased appetite. The effectiveness of the treatment may depend upon the stage at diagnosis.
NOTE: Treatment Options listed below are not all-inclusive. Other treatments may be available. ChemoExperts provides drug information and does not recommend any one treatment over another. Only your Doctor can choose which therapy is appropriate for you.
What is a "17p deletion"?
A blood test is used to detect the mutation known as a “17p deletion.”
The genetic material which makes up the small arm (also known as “p” for petit) of Chromosome 17, is where the gene known as “the guardian of the genome” lives. When this gene is missing on 17p, this condition is often referred to as a 17p deletion. If this deletion is detected, the leukemia may behave more aggressively. Click for more information on mutation testing.
What does “low risk” mean?
Low risk patients can usually be managed in an outpatient clinic. These are patients who have small lymph nodes (less than 5 cm or about 2 inches), and few CLL cells in the blood (less than 25 thousand per microliter).
Patients with “low risk” CLL should still receive IV hydration when starting venetoclax, as well as an oral medication known as allopurinol to protect the kidneys.
What does “medium risk” mean?
Medium risk patients can usually be managed in an outpatient clinic. These are patients who have slightly larger lymph nodes (between 5 - 10 cm, or about 2 - 4 inches), or many CLL cells in the blood (more than 25 thousand per microliter), but not both.
Patients with “medium risk” CLL should receive IV hydration when starting venetoclax, as well as an oral medication known as allopurinol to protect the kidneys. Patients with kidney problems, or elderly patients may need to be hospitalized for the first day or two when starting the 20 mg or 50 mg doses.
What does “high risk” mean?
High risk patients SHOULD be managed in the hospital for the first day or two when starting the 20 mg or 50 mg doses. These are patients who have a large lymph node (greater than 10 cm, or about 4 inches), or many CLL cells in the blood (more than 25 thousand per microliter), plus a slightly larger lymph node (greater than 5 cm, or about 2 inches).
Patients with “high risk” CLL should receive IV hydration when starting venetoclax, as well as an oral medication known as allopurinol to protect the kidneys, and sometimes an IV medication known as rasburicase to further protect the kidneys.
Starter Pack Dosing
The Venetoclax Starter Pack includes the following:
Week 1: Venetoclax 20 mg (two 10 mg tabs) by mouth once daily = fourteen 10 mg tablets
Week 2: Venetoclax 50 mg by mouth once daily = seven 50 mg tablets
Week 3: Venetoclax 100 mg by mouth once daily = seven 100 mg tablets
Week 4: Venetoclax 200 mg (two 100 mg tabs) by mouth once daily = fourteen 100 mg tablets
Of note: Week 5 and beyond: 400 mg (four 100 mg tabs) by mouth once daily are dispensed as a separate prescription as a one month supply
Important: Tablets should be kept in their original container until use.
Clinical Studies
If you are interested in reading the clinical trials results, please click on reference below:
Roberts AW, Davids MS, Pagel JM, et al. Targeting BCL2 with venetoclax in relapsed chronic lymphocytic leukemia. N Engl J Med. 2016;374:311-322.
What is a CBC?
A Complete Blood Count (CBC) is a frequently ordered blood test that tells clinicians the status of your: 1) White blood cell count, 2) Hemoglobin, and 3) Platelet count at the time the test was taken.
Common uses:
1) White blood cell count (WBC): is used to determine infection risk, or response to chemotherapy. Certain chemotherapy agents may harm our good infection-fighting cells. Sometimes chemotherapy may need to be delayed to allow these cells to recover.
2) Hemoglobin: is used to determine if someone is anemic. Anytime the hemoglobin is below 12 g/dL, the person is said to be anemic. Red blood cell transfusions, and sometimes iron can be given to restore the hemoglobin level, but anemia treatment should always aim at treating the underlying cause or condition.
3) Platelet count: is used to determine if the risk of bleeding is increased or if a platelet transfusion is required to prevent bleeding. Certain medications that increase bleeding risk, such as: aspirin, certain chemotherapy agents, and blood thinners, may need to be stopped temporarily until the platelet count is within a safe range.
What is a CMP?
A Comprehensive Metabolic Panel (CMP) is a frequently ordered blood test that tells clinicians the status of your: 1) Electrolytes & Acid/Base status, 2) Kidney function, 3) Liver function, 4) Blood sugar, and 5) Calcium at the time the test was taken. It is commonly used to monitor liver and kidney function when beginning new medications such as chemotherapy. A total of 14 tests are run simultaneously and are shown below.
Electrolytes & Acid/Base status:
1) Sodium, 2) Potassium, 3) Carbon dioxide, 4) Chloride
Kidney Function:
5) BUN (blood urea nitrogen), 6) Serum creatinine (Scr)
Liver Function:
7) AST, 8) ALT, 9) Total bilirubin, 10) Alk Phos, 11) Albumin, 12) Total protein
Blood sugar:
13) Serum glucose
Calcium:
14) Serum calcium
What is Tumor Lysis Syndrome?
Tumor lysis syndrome occurs when many cancer cells die quickly and release their contents into the bloodstream. Many times the body has the ability to flush these substances out through the kidneys or metabolize them via the liver. However, sometimes the body needs medicines to help eliminate these substances and to prevent organ damage.
These medicines may include: IV hydration, oral allopurinol, IV rasburicase, plus others
